Could Hammer Toes Trigger Leg Ache
 Overview
Overview
hammertoes is the general term used to describe an abnormal contraction or "buckling" of the toe because of a partial or complete dislocation of one of the joints of the toe or the joint where the toe joins with the rest of the foot. As the toe becomes deformed, it rubs against the shoe and the irritation causes the body to build up more and thicker skin to help protect the area. The common name for the thicker skin is a corn.
Causes
The most common cause of hammertoe is a muscle/tendon imbalance. This imbalance, which leads to a bending of the toe, results from mechanical (structural) changes in the foot that occur over time in some people. Hammertoes may be aggravated by shoes that don?t fit properly. A hammertoe may result if a toe is too long and is forced into a cramped position when a tight shoe is worn. Occasionally, hammertoe is the result of an earlier trauma to the toe. In some people, hammertoes are inherited.
 Symptoms
Symptoms
People with a hammer toe will often find that a corn or callus will develop on the top of the toe, where it rubs against the top of the footwear. This can be painful when pressure is applied or when anything rubs on it. The affected joint may also be painful and appear swollen.
Diagnosis
First push up on the bottom of the metatarsal head associated with the affected toe and see if the toe straightens out. If it does, then an orthotic could correct the problem, usually with a metatarsal pad. If the toe does not straighten out when the metatarsal head is pushed up, then that indicates that contracture in the capsule and ligaments (capsule contracts because the joint was in the wrong position for too long) of the MTP joint has set in and surgery is required. Orthotics are generally required post-surgically.
Non Surgical Treatment
People with a hammer toe benefit from wearing shoes in which the toe box is made of a flexible material and is wide enough and high enough to provide adequate room for the toes. High-heeled shoes should be avoided, because they tend to force the toes into a narrow, flat toe box. A doctor may recommend an insert (orthotic) for the shoe to help reduce friction and pressure on the hammer toe. Wearing properly fitted shoes may hammertoe reduce pain and inflammation. It may also prevent ulcers from developing and help existing ulcers heal. However, the hammer toe does not disappear.
Surgical Treatment
Sometimes, if the deformity is severe enough or surgical modification is needed, the toe bones may be fused so that the toe does not bend. Buried wires are used to allow for the fusion to heal, and they remain in place after healing. Your skin is closed with fine sutures, which are typically removed seven to ten days after surgery. A dressing is used to help keep your toes in their new position. Dressings should not get wet or be removed. After surgery, your doctor may prescribe pain relievers, typically for the initial four to seven days. Most people heal completely within one month of surgery, with few complications, if any. Crutches or a cane may be needed to help you keep weight off your affected foot, depending on the procedure. Occasionally, patients receive a special post-op shoe or a walking boot that is to be worn during the healing process. Most people are able to shower normally after surgery, but must protect the dressing from getting wet. Many patients are allowed to resume driving within one week after the procedure, but care needs to be taken.
Bilateral Hallux Valgus Deformity
Overview
 A bunion is generally considered as an enlargement of the joint (a lump of bone) at the base and side of the big toe (specifically, the first metatarsophalangeal joint). Bunions form when the toe moves out of place. As the big toe bends towards the others this lump becomes larger and the bunion can become painful, arthritis and stiffness can eventually develop. Hallux valgus or hallux abducto valgus (HAV) is the name used for the deviated position of the big toe and a bunion refers to the enlargement of the joint, most of the time the two go together and can just be referred to as 'bunions'. The word bunion is from the Latin "bunion," meaning enlargement.
A bunion is generally considered as an enlargement of the joint (a lump of bone) at the base and side of the big toe (specifically, the first metatarsophalangeal joint). Bunions form when the toe moves out of place. As the big toe bends towards the others this lump becomes larger and the bunion can become painful, arthritis and stiffness can eventually develop. Hallux valgus or hallux abducto valgus (HAV) is the name used for the deviated position of the big toe and a bunion refers to the enlargement of the joint, most of the time the two go together and can just be referred to as 'bunions'. The word bunion is from the Latin "bunion," meaning enlargement.
Causes
Women traditionally have a higher rate of bunions, which is to be expected, since it is they who have traditionally worn shoes with high heels, a narrow toe box, or whatever fashion dictates from year to year. However, men can suffer from bunions as well, as can anyone for whom the right (or wrong) conditions exist, poor foot mechanics, improper footwear, occupational hazards, health and genetic predisposition. Finally, bunions have long been a condition associated with the elderly, and although they often appear in conjunction with inflammatory joint diseases such as arthritis (which is often associated with age), they can strike at any point in life, including adolescence.
Symptoms
The most obvious symptoms of a bunion are. Pain in the area of the MTP joint, the joint where your big toe connects to your foot. Bending of the big toe in towards the other toes. An enlarged bump of bone or tissue at the MTP joint. Each symptom can range in degree from small to severe. Sometimes the pain can be sufficient to make it difficult to walk in normal shoes. Other symptoms may include. Swelling and inflammation of the skin around the MTP joint. Thickening of the skin in the area of the joint. Restricted motion in your big toe. Pressure from the inward bending of your big toe can affect your other toes, leading to corns on your smaller toes. Ingrown toenails on the smaller toes. Development of hammertoes in the other toes. Calluses on the bottom of your foot. If you have any of these symptoms, especially pain, displacement of your big toe or development of a bulge, you should consider consulting your physician. Even if you're not significantly bothered by some of these symptoms, bunions tend to continue getting bigger and more serious over time and should be taken care of before they do so.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
Wear comfortable shoes that don't squeeze your toes together. Sandals are ideal in warm weather. Cushioning the bunion with a donut-shaped bunion pad sold at drugstores can prevent any direct rubbing against your shoes. Have your shoes stretched to give your foot more room or consider switching to footwear customized to relieve pressure on the affected area. Soak your foot in warm water to help lessen the pain after a day on your feet. Apply ice packs several times a day to reduce swelling of painful and inflamed bunions. Take aspirin or ibuprofen for the inflammation and pain, and try supplementing with anti-inflammatory herbs such as ginger and turmeric (these work more slowly than the drugs). See a podiatrist for specially fitted shoes or orthotic devices that may help. Sometimes, surgery is necessary. Seek a second opinion before scheduling any operation. 
Surgical Treatment
Surgery might be recommended if non-surgical treatments fail to provide relief, and you are having trouble walking or are in extreme pain. Surgery can be used to return the big toe to its correct anatomical position. During surgery, bones, ligaments, tendons, and nerves are put back into correct order, and the bump is removed. Many bunion correction procedures can be done on a same-day basis. The type of procedure will depend on your physical health, the extent of the foot deformity, your age, and your activity level. The recovery time will depend on which procedure or procedures are performed. Surgery may be recommended to correct a tailor?s bunion, but is unlikely to be recommended for an adolescent bunion.
Overpronation Of The Feet Painfulness
Overview
Over Pronation (Flat Feet) refers to the biomechanical shock-absorbing motion of the ankle, foot and lower leg. It is the natural inward flexing motion of the lower leg and ankle. Standing, walking, and running cause the ankle joint to pronate which in turn helps the body to absorb shock and allows it to control balance. An ankle joint that is too flexible causes more pronation than desired. This common condition is called Over- Pronation (sometimes referred to as "Flat Feet"). This foot condition places an extreme degree of strain on various connective tissues of the ankle, foot, and knee. If this condition is not addressed foot pain and toe deformities such as bunions and hammer toes (just to name a couple) may develop. Hip and lower back pain may also be residual results from this condition.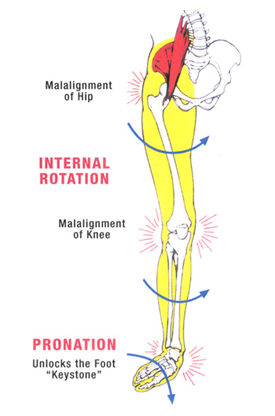
Causes
A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development.
Symptoms
Overpronation can negatively affect overall body alignment. The lowering of the longitudinal arch pulls the heel bone in, causing the leg, thigh bone and hip to rotate inwards, and an anterior tilt of the pelvis. Unnecessary strain to the ankles, knees, hips and back can result. Plantar fasciitis and inflammation, metatarsal pain, problems with the Achilles tendon, pain on the inside of the knee, and bursitis in the hip are just some of the conditions commonly associated with pronation.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Supportive orthotics in the shoe is a method commonly implemented to treat many common running injuries associated with pronation. An advantage of orthotics is that they often allow the sufferer to continue to participate in athletic activity and avoid other treatment options that could be potentially costly and time consuming. Seventy-five percent of injured runners are successfully treated with the prescription of orthoses. Orthotics are the most effective treatment for symptoms that develop from unusual biomechanics within the body such as overpronation, resulting in either great improvement or complete healing of the injury in about half the cases.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Over Pronation (Flat Feet) refers to the biomechanical shock-absorbing motion of the ankle, foot and lower leg. It is the natural inward flexing motion of the lower leg and ankle. Standing, walking, and running cause the ankle joint to pronate which in turn helps the body to absorb shock and allows it to control balance. An ankle joint that is too flexible causes more pronation than desired. This common condition is called Over- Pronation (sometimes referred to as "Flat Feet"). This foot condition places an extreme degree of strain on various connective tissues of the ankle, foot, and knee. If this condition is not addressed foot pain and toe deformities such as bunions and hammer toes (just to name a couple) may develop. Hip and lower back pain may also be residual results from this condition.
Causes
A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development.
Symptoms
Overpronation can negatively affect overall body alignment. The lowering of the longitudinal arch pulls the heel bone in, causing the leg, thigh bone and hip to rotate inwards, and an anterior tilt of the pelvis. Unnecessary strain to the ankles, knees, hips and back can result. Plantar fasciitis and inflammation, metatarsal pain, problems with the Achilles tendon, pain on the inside of the knee, and bursitis in the hip are just some of the conditions commonly associated with pronation.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
Supportive orthotics in the shoe is a method commonly implemented to treat many common running injuries associated with pronation. An advantage of orthotics is that they often allow the sufferer to continue to participate in athletic activity and avoid other treatment options that could be potentially costly and time consuming. Seventy-five percent of injured runners are successfully treated with the prescription of orthoses. Orthotics are the most effective treatment for symptoms that develop from unusual biomechanics within the body such as overpronation, resulting in either great improvement or complete healing of the injury in about half the cases.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Coping With Calcaneal Apophysitis
Overview
Sever?s disease (also known as calcaneal apophysitis) is a type of bone injury in which the growth plate in the lower back of the heel, where the Achilles tendon (the heel cord that attaches to the growth plate) attaches, becomes inflamed and causes pain. Sever?s disease is the most common cause of heel pain in children, especially those who exercise or play sports on a regular basis.
Causes
Severs disease is caused by repetitive excessive force to the growing area of the heel bone, causing injury to this area. The calf muscles (soleus and gastrocnemius) are attached by the Achilles tendon to the calcaneus (heel bone). They exert a huge force during running , jumping and landing. In children, there is a growing area in the heel bone called the apophysis and is made of relatively weak cartilage. If there is excessive force at this relatively weak point damage occurs. This excess force can be caused by a number of factors. During the adolescent growth spurt the bones grow very quickly. The muscles do not grow out at the same rate as the bone grows and so can become very tight. The calf muscles generate huge forces when they are used to run, jump and land. This force is transmitted to the calcaneal apophysis (growth area). The gastrocnemius muscle spans both the ankle and knee joint. Tightness of this or any other muscles of the lower limb (hamstring or quadriceps) cause extra force at the growing (weak) area. In active children, who undertake a lot of exercise, the repetitive high force causes damage. If your child has poor biomechanics due to poor lower limb alignment (often caused by flat feet), the muscles of the lower limb have to work excessively hard and this can cause increased force at the tibial tubercle.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
Sever?s disease (also known as calcaneal apophysitis) is a type of bone injury in which the growth plate in the lower back of the heel, where the Achilles tendon (the heel cord that attaches to the growth plate) attaches, becomes inflamed and causes pain. Sever?s disease is the most common cause of heel pain in children, especially those who exercise or play sports on a regular basis.
Causes
Severs disease is caused by repetitive excessive force to the growing area of the heel bone, causing injury to this area. The calf muscles (soleus and gastrocnemius) are attached by the Achilles tendon to the calcaneus (heel bone). They exert a huge force during running , jumping and landing. In children, there is a growing area in the heel bone called the apophysis and is made of relatively weak cartilage. If there is excessive force at this relatively weak point damage occurs. This excess force can be caused by a number of factors. During the adolescent growth spurt the bones grow very quickly. The muscles do not grow out at the same rate as the bone grows and so can become very tight. The calf muscles generate huge forces when they are used to run, jump and land. This force is transmitted to the calcaneal apophysis (growth area). The gastrocnemius muscle spans both the ankle and knee joint. Tightness of this or any other muscles of the lower limb (hamstring or quadriceps) cause extra force at the growing (weak) area. In active children, who undertake a lot of exercise, the repetitive high force causes damage. If your child has poor biomechanics due to poor lower limb alignment (often caused by flat feet), the muscles of the lower limb have to work excessively hard and this can cause increased force at the tibial tubercle.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
Achilles Tendon Reconstruction Cpt Code
Overview
 Achilles tendon rupture are common. Most athletes describe a sudden acute event with an associated popping sensation and pain in the Achilles tendon. They often think that they have been kicked or struck in the calf. It is important to get prompt treatment and to be placed in an equinous cast (a cast with the foot in a pointed position). More definitive treatment options can be discussed after this has occurred.
Achilles tendon rupture are common. Most athletes describe a sudden acute event with an associated popping sensation and pain in the Achilles tendon. They often think that they have been kicked or struck in the calf. It is important to get prompt treatment and to be placed in an equinous cast (a cast with the foot in a pointed position). More definitive treatment options can be discussed after this has occurred.
Causes
The causes of an Achilles tendon rupture are very similar to Achilles tendinitis. Causes include. Running uphill. Running on a hard surface. Quickly changing speeds from walking to running. Playing sports that cause you to quickly start and stop.
Symptoms
The most common initial symptom of Achilles tendon rupture is a sudden snap at the back of the heels with intense pain. Immediately after the rupture, the majority of individuals will have difficult walking. Some individuals may have had previous complains of calf or heel pain, suggesting prior tendon inflammation or irritation. Immediately after an Achilles tendon rupture, most individuals will develop a limp. In addition, when the ankle is moved, the patient will complain of pain. In all cases, the affected ankle will have no strength. Once the Achilles tendon is ruptured, the individual will not be able to run, climb up the stairs, or stand on his toes. The ruptured Achilles tendon prevents the power from the calf muscles to move the heel. Whenever the diagnosis is missed, the recovery is often prolonged. Bruising and swelling around the calf and ankle occur. Achilles tendon rupture is frequent in elderly individuals who have a sedentary lifestyle and suddenly become active. In these individuals, the tendon is not strong and the muscles are deconditioned, making recovery more difficult. Achilles tendon rupture has been reported after injection of corticosteroids around the heel bone or attachment of the tendon. The fluoroquinolone class of antibiotics (such as ciprofloxacin [Cipro]) is also known to cause Achilles tendon weakness and rupture, especially in young children. Some individuals have had a prior tendon rupture that was managed conservatively. In such cases, recurrence of rupture is very high.
Diagnosis
Other less serious causes of pain in the back of the lower leg include Achilles tendonitis or bursitis. To distinguish between these possibilities, your physician will take a thorough history and examine your lower leg to look for signs of a rupture. The presence of a defect in the tendon that can be felt, evidence of weakness with plantarflexion, and a history consistent with Achilles tendon rupture are usually sufficient for diagnosis. Your physician may also perform a ?Thompson test,? which consists of squeezing the calf muscles of the affected leg. With an intact Achilles tendon, the foot will bend downward; however, with a complete rupture of the tendon, the foot will not move. In cases where the diagnosis is equivocal, your physician may order an MRI of the leg to diagnose a rupture of the Achilles tendon.
Non Surgical Treatment
A medical professional will take MRI scans to confirm the diagnosis and indicate the extent of the injury. Sometimes the leg is put in a cast and allowed to heal without surgery. This is generally not the preferred method, particularly for young active people. Surgery is the most common treatment for an achilles tendon rupture. 
Surgical Treatment
Your doctor may recommend surgery if you?re young and active, or an athlete. However, this will depend on where your tendon is ruptured. If the rupture is at, or above, the point at which your tendon merges with your calf muscle, for example, surgery may not be possible. There are three main types of surgery to repair a ruptured Achilles tendon. Open surgery. Your surgeon will make one long cut in your leg to reach the tendon and repair it. Limited open surgery. Your surgeon will still make a single cut but it will be shorter. Percutaneous surgery. Your surgeon will make a number of small cuts to reach the tendon and repair it. In all types of surgery, your surgeon will stitch the tendon together so it can heal. Each type of surgery has different risks. Open surgery is less likely to injure one of the nerves in your leg for example, but has a higher risk of infection. Ask your surgeon to explain the risks in more detail. After your operation, you will need to wear a series of casts or an adjustable brace on your leg to help your Achilles tendon heal. This will usually be for between four and eight weeks. There is a chance that your tendon will rupture again after the operation.
Prevention
To prevent Achilles tendonitis or rupture, the following tips are recommended. Avoid activities that place an enormous stress on the heel (for example, uphill running or excessive jumping). Stop all activity if there is pain at the back of the heel. If pain resumes with one particular exercise, another exercise should be selected. Wear proper shoes. Gradually strengthen calf muscles with sit-ups if prior episodes of Achilles tendonitis have occurred. Always warm up with stretching exercises before any activity. Avoid high-impact sports if prior episodes of Achilles tendon injury.